
Early COVID patient beats the odds, matches “dreamworld” experience to reality
Anoop Chugh was one of Hamilton Health Sciences’ (HHS) first very sick COVID-19 patients to “make it.”
He was admitted to Juravinski Hospital on March 28, 2020 – early on in the first wave of the pandemic.
Chugh was so ill, his care required a ventilator and life support. He was sedated, paralyzed and proned – the latter two are only done to the sickest patients in order to turn them from their back to their stomach to help with breathing.
To say he went through a lot is an understatement.
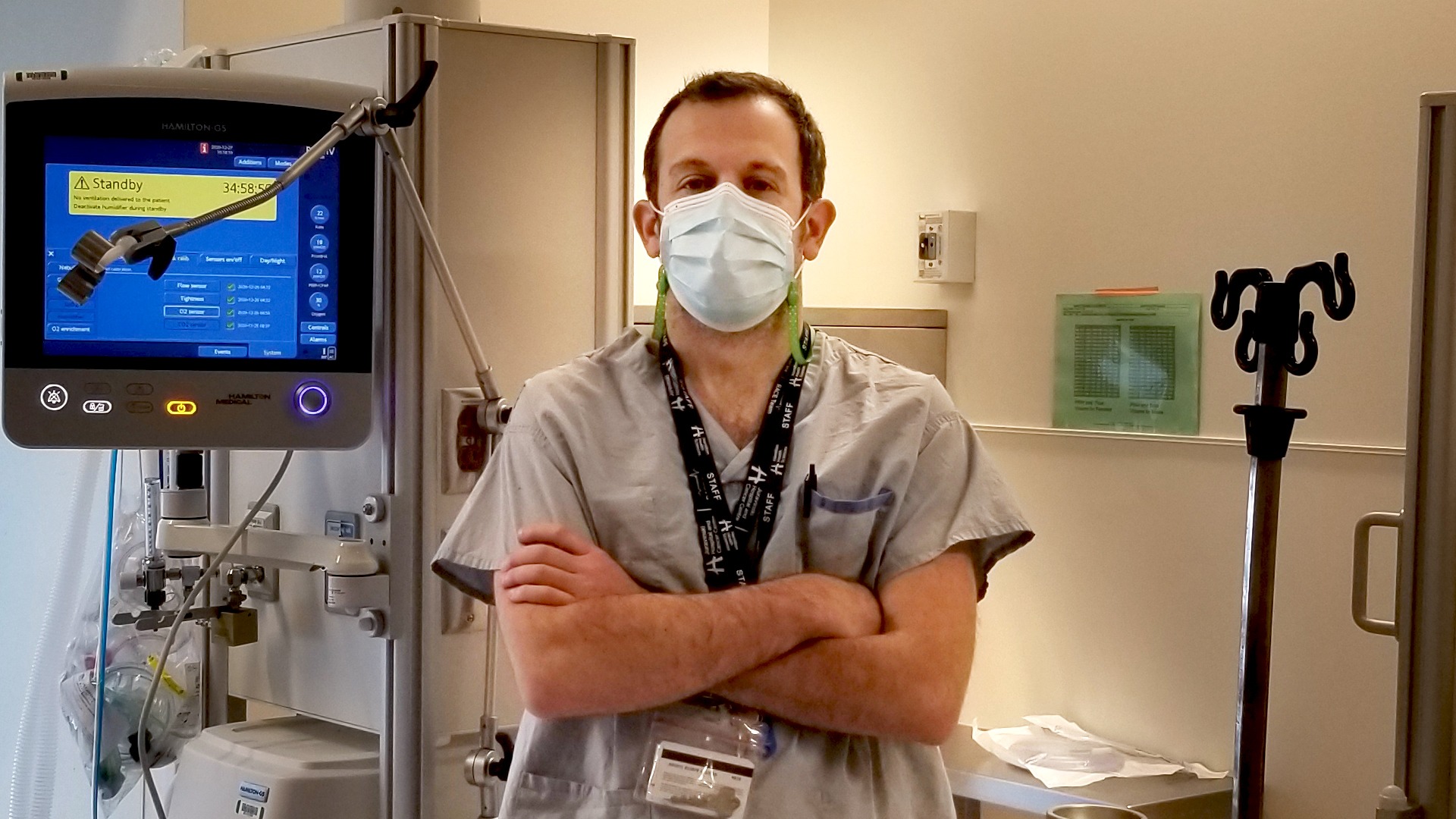
Bram Rochwerg
“He was very ill and the odds were stacked against him,” says Juravinski Hospital intensive care doctor Bram Rochwerg. “There is no doubt there were many times that he was doing poorly and we thought he wouldn’t make it through.”
But he did.
“Life in the dream world”
Chugh contracted COVID-19 around March 15, 2020 – he isn’t sure how. It started as a tickle in his throat and progressed to trouble breathing so he called an ambulance.
A couple of days into his hospital stay he was sedated in order to place a tube down his throat to help with his breathing. He woke up a month later.
“Even though I was out, I could tell what was happening in real life. A lot of it was making it into my dreams,” he remembers. “It’s been a year now but I remember all of it vividly. For me, it was life in the dream world. When I heard about what happened at a particular point, I was able to correlate it to what was happening in my dreams.”
He says he felt helpless.
After effects
Chugh was transferred from Juravinski Hospital to Hamilton General Hospital when HHS was trying to keep all COVID-19 patients in one location (this later changed as the number of COVID-19 patients grew). Around this time, he woke up as sedation was turned off and he was able to come off the ventilator.
He was weak.
“I couldn’t open a cereal box. I couldn’t talk because I had a tracheostomy in. I couldn’t write because my hands were too weak to hold a pen. Communicating was extremely difficult.”
It took a couple of weeks before Chugh was semi-independent – but that was just his upper body.
During his time in hospital, he contracted Guillain-Barré syndrome, a serious health condition that occurs when the body’s immune system mistakenly attacks part of the nervous system causing muscle weakness or paralysis.
“My foot and leg would fire up with so much pain,” he says. Previously healthy, Chugh had to relearn many mobility basics such as how to balance, walk, and climb stairs. “You don’t go in thinking you’ll come out not being able to do things you took for granted your entire life.”
Chugh moved to HHS’ Regional Rehabilitation Centre for a couple of weeks to work with the rehab team on walking, showering, and being independent.
“They had me up using a cane again in no time,” he says. “They have a fantastic program.”
A long road to recovery at home

Anoop surprises his son on Father’s Day
Chugh went home on June 19, 2020 – just in time to surprise his son for Father’s Day.
The 47-year-old is continuing physiotherapy at home to regain strength in his leg and foot. He still suffers from Guillain-Barré syndrome. He has no feeling in his left foot and is unable to curl his toes. He has been told it can take up to three years for the nerves to regenerate.
He sometimes experiences trouble sleeping.
His mental health is good – but he can understand the immense toll an experience like this can take on a person’s mental health.
But his biggest takeaway is the toll a prolonged hospital stay takes on the physical body, even for somebody who is relatively young and healthy to start.
“You don’t really realize just how much lying in bed affects you. I couldn’t raise my hand over my head,” he says. “It took the better part of 6-8 months until I started to get back to some semblance of normal.”
Post-intensive care syndrome
Physical challenges are just one of the consequences intensive care unit (ICU) survivors may experience.
The long-term consequences of an ICU stay has been referred to as “post-intensive care syndrome” or PICS. PICS can have significant impacts on a patient’s physical, cognitive and mental health.
“Post-intensive care syndrome is a real thing, increasingly being recognized clinically and in the research setting over the last five to ten years,” says Rochwerg. “COVID, like any other cause of critical illness, can certainly lead to PICS. And given the large volume of critically ill patients we have had in Ontario these past few months because of COVID, I do anticipate this will lead to a burden on our healthcare system for months and years to come.”
A recent study Rochwerg contributed to shows that survivors of critical illness in Ontario have higher rates of mental health challenges and suicide following their ICU stay.
Some effort is being made in the HHS ICU to decrease the risk of PICS, such as encouraging people to move their bodies as early as possible (such as early physiotherapy and new tools like in-bed cycling for ventilated patients), emphasizing family-centered care, and involving social workers to work with patients and their families on stress management and coping skills.
Keeping an “ICU diary” is another strategy used to decrease the risk of PICS by documenting a patient’s experience.
Chugh’s wife and sister kept a diary that contains a mix of medical information and personal reflections.
“It definitely filled in a lot of gaps helping me to realize what happened and at what particular time,” he says.
“Making sure that I lived”
While Chugh was sedated, he remembers a nurse asking the doctor in his room if they were going home for the night.
“I heard the doctor say, ‘No, I want to stay to make sure he can make it through the night.’ And that sums up the level of care that I got,” he says. “There were so many people who devoted themselves to making sure that I lived. I can’t thank them enough.”


